

If you’ve been told you have an “extra vertebra” or a disc between S1 and S2, you may have a condition known as lumbarisation of S1.
Many people in Perth discover this finding incidentally on MRI or X-ray. Some are told it’s irrelevant. Others are told it explains everything.
So what’s the truth?
At Perth Injury & Pain Clinic, we assess lumbarisation through a biomechanical, load-focused lens — focusing not just on anatomy, but on how your spine is being stressed during daily life.
Let’s break it down clearly.
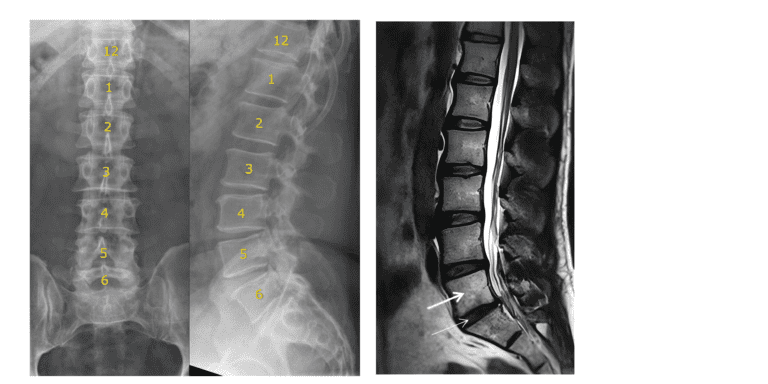
Lumbarisation is a type of lumbosacral transitional vertebra (LSTV).
Normally, the spine consists of:
With lumbarisation:
This anatomical variation is relatively common, with studies estimating prevalence anywhere from 4% to 30% of the population.
Most people never know they have it.
The short answer:
Not always — but it can contribute.
Peer-reviewed research (Castellvi 1984; Bron 2007; Apazidis 2011; Luoma 2004) shows that certain types of transitional vertebrae are associated with:
This is sometimes referred to as Bertolotti’s Syndrome.
However, imaging findings alone do not equal pain.
What matters most is:
👉 How the spine is functioning
👉 How it is being loaded
👉 Whether certain tissues are sensitised
From a biomechanical perspective, lumbarisation may:
Research in spinal biomechanics consistently demonstrates that:
If lumbarisation alters how forces travel through the lumbosacral region, it may increase stress on:
Over time, this can contribute to:
Many people come to us after being told they have back pain and a scan report stating they have a lumbarisation – but not told how this may contribute to their issues or how to rehab it. That is because very few have undergone a detailed assessment.

Because the label “lumbarisation” doesn’t tell us what to fix.
Movement does
Treatment is not about “correcting” the anatomy. It’s about improving how the spine handles load.
This may include:
Eliminating repeated loaded flexion
Modifying gym exercises
Adjusting sitting posture
Reducing prolonged static positions
Improving daily movement strategies
Rehabilitation often focuses on:
Enhancing abdominal wall endurance
Developing effective bracing strategies
Encouraging hip-driven movement
Improving segmental control
This reduces excessive micro-movement and shear stress at sensitised segments.
If the lower lumbar spine is under increased stress:
The hips must absorb more motion
Thoracic mobility becomes essential
Pelvic control becomes critical
Many cases of persistent low back pain improve significantly once movement patterns are optimised and load exposure is managed correctly.
Surgery for lumbarisation is extremely rare. The vast majority can be addressed with targeted, non-operative rehabilitation.
What it is:
• A structural variation
• Common in the general population
• Not automatically a cause of pain
But in the presence of:
• Repeated mechanical stress
• Poor load tolerance
• Endplate or disc sensitivity
• Asymmetrical shear
It can contribute to ongoing low back pain.
The key is not chasing the scan.
The key is understanding how your spine is being loaded.
If you’ve been diagnosed with:
And you still don’t feel like you’ve had a clear mechanical explanation…
At Perth Injury & Pain Clinic, we provide:
Our approach focuses on identifying why your pain persists — and building a plan around that.
What if your back pain isn’t just from one bad movement — but from constantly living on the edge of your spine’s limits? This is
One of the most overlooked causes of persistent low back pain is how we move during everyday tasks. Simple activities like bending, sitting, getting out of a car, or